
The ultimate irony of my diagnosis is that I had it right all along.
I self-diagnosed correctly at the very beginning, but it still took a year and a half to get a formal diagnosis from a medical professional.
My disease is only seen in a small handful of people across the nation – roughly 1-5 people per million. This means that most doctors, including experienced specialists, will go an entire career without ever seeing a case. And if they do see a case in a patient, chances are high that they’ll have no idea what they’re looking at and misdiagnose.
This was the case for me.
I walked into my primary care doctor’s office in the spring of 2023 with severe mouth ulcers. When I say severe – I mean I couldn’t eat solid food without my flesh breaking apart as I chewed and swallowed. It even hurt to drink water because my esophagus was covered with open, bleeding sores. I had been obsessively searching Google for answers. I had self-diagnosed a very rare autoimmune disease called pemphigus vulgaris. It seemed like an exact match based on the articles and photos I was finding, so I asked ‘Could it be this?‘
Lots of doctors would roll their eyes over a rare disease, but my primary care doctor is open-minded. He didn’t shoot me down. He searched his database of labs to see if there was bloodwork that could be performed.
There is bloodwork for pemphigus. Unfortunately (and unbeknownst to my PCP), it’s not a diagnostic test.
In reality, a definitive pemphigus diagnosis can only be made by biopsy. Dermatology is the specialty that performs these biopsies and treats pemphigus.
In mid-August of 2023, I went to see a dermatologist about my illness.
We had a long discussion about different autoimmune conditions that cause mouth ulcers and sores. We talked about pemphigus, lichen planus, and lupus (among other things.) She suggested that I might have better luck getting an accurate diagnosis with a rheumatologist, but briefly mentioned performing biopsies if symptoms didn’t resolve.
When I originally saw this dermatologist, I did not have portal access at their practice. I only ever saw my visit notes over a year later when they opened the system to patient logins. I was stunned at what I found in her notes from my initial visit.
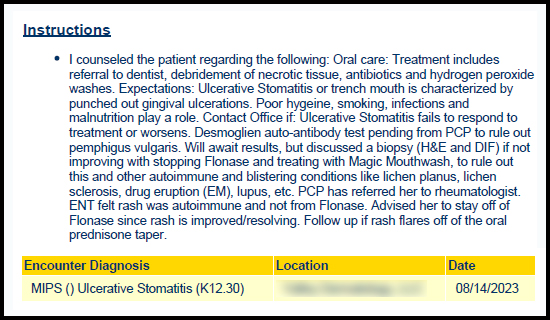
She thought I might have trench mouth??? She never said that to my face. She never suggested debridement or poor oral hygiene to me. Malnutrition – no way! Smoking – never ! If she had asked me any questions, I would have told her I have impeccable oral hygiene. I’ve had one cavity in my life and my dentist praises my healthy teeth and gums on every visit. I can’t believe this went into my permanent medical record without it ever being mentioned to me.
Ulcerative stomatitis, an umbrella term for mouth ulcers, was another possibility she listed.
The main thing worth noting from this first visit was that she knew that both DIF and H&E biopsies are the standard tests performed for the diagnosis of autoimmune blistering disorders. They should have been part of her routine diagnostic steps from the very beginning. She also had no clue that the desmoglein auto-antibody bloodwork is not a diagnostic tool. She didn’t even know how to spell desmoglein!
As you’ve probably guessed, my symptoms did not resolve and I returned to dermatology in January of 2024. I personally requested the biopsies to rule out pemphigus. I still thought it might be a possibility.
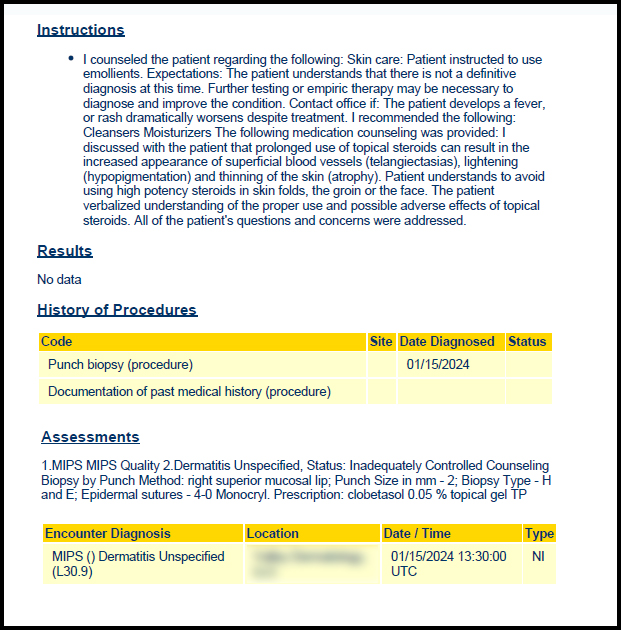
The takeaway to note from the biopsy visit is that the dermatologist only sent the sample for H&E interpretation – no direct immunofluorescence (DIF) biopsy at all.
As the patient, I assumed she knew what she was doing. I had never had biopsies before and assumed the samples she collected would be used for both types of biopsy.
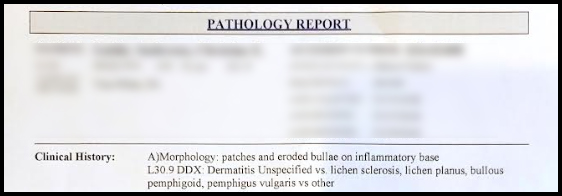
Even the order she wrote to pathology indicated that the purpose of the biopsy was to rule out a variety of autoimmune blistering diseases.
I feel she failed me completely. She did not do what she said she would do or perform her job to the basic standard of care indicated in such a situation. The consequences and harm she caused were devastating to me and my family.
Without the direct immunofluorescence biopsy, the pathology was mis-read. I was told I had cold sores and sent home with a prescription for Valtrex. I’d never had a cold sore in my life before this.
A herpes simplex infection (HSV1 or cold sores) is actually one of the most common misdiagnoses in pemphigus patients. I am not the only person this has happened to.
This misleading biopsy ended up sending all my healthcare providers down so many dead-end rabbit holes. They believed pemphigus had been ruled out. When my symptoms only got worse on Valtrex, they were baffled but agreed something bigger was probably going on. They continued to make guess after guess, before finally labeling my condition as erosive lichen planus, while admitting they still weren’t really sure.
With that diagnosis, I began researching my own specialists. I wasn’t happy with the treatment plan. I wasn’t feeling any better. Nothing was working and I was getting mucosal ulcers other places beyond my mouth. Life as a medical mystery was harrowing.
Through a Facebook group of lichen planus patients, I found that there was an autoimmune blistering diseases lab at UNC Chapel Hill Medical Center. There was an experienced specialist practicing in the dermatology clinic. They did research and drug trials. They saw other patients like ME! I asked my rheumatologist for a referral.
UNC called me back almost immediately to schedule a consult. A few weeks later, I had two biopsies – the ones I should have had all along. The day after the biopsies, I got a call – ‘You have a disease called pemphigus.’
My response – I KNEW IT!
I am extremely grateful for the diagnosis, but frustrated it took me so long to get there. It stings to know I had my diagnosis in mind from the beginning, but it still got missed. I can only dream of what it would have been like to be treated earlier and to have suffered less.
But, I am here now and ready to tackle this illness. There is treatment. There is hope. I can dream of remission.
